

The Deep Front Myofascial Arm Line in Clinical Practice
Myofascial Continuity from the Rib Cage to the Thumb
The Deep Front Myofascial Arm Line in Clinical Practice
Myofascial Continuity from the Rib Cage to the Thumb
Healthcare professionals rely heavily on their thumbs throughout the workday. Dentists, dental assistants, hygienists, physiotherapists, surgeons, and manual therapists depend on them for precision grip, stabilization, and controlled pressure.
The thumb does not function independently. Through the Deep Front Myofascial Arm Line, a continuous pathway links the lateral chest, shoulder blade, upper arm, forearm, and thumb into one integrated system.
Within this line, the pectoralis minor plays an especially important role. This small but influential muscle attaches to the coracoid process of the scapula and strongly affects how the shoulder blade positions and moves.
When the pectoralis minor becomes shortened or over-recruited—something common in professions that work with the arms forward—the scapula can elevate and rotate around the upper ribs toward the front of the body. As a result, tension can transmit down the Deep Front Arm Line and increase load through the forearm and thumb, often contributing to compression within the carpal tunnel.
For clinicians whose work depends on repetitive precision with the hands, maintaining mobility and adaptability along this pathway becomes essential.
Deep Front Myofascial Arm Line (DFAL)
The Deep Front Arm Line begins along the anterior ribs and travels down the front of the arm toward the thumb side of the forearm and hand.
Key structures within this line include the 1. pectoralis minor, 2. clavipectoral fascia, 3. subclavius, 4. biceps brachii, 5/6. radial periosteum, 7. radial collateral ligaments, and 8/9. thenar musculature at the base of the thumb.
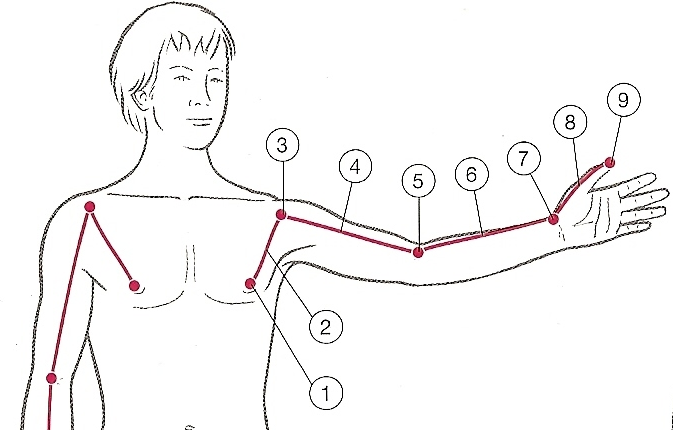
Together, these structures form a continuous myofascial pathway linking the lateral chest and shoulder blade to the full arm and thumb.
Because this pathway continues directly into the thumb, changes higher in the chain—particularly around the pectoralis minor and scapula—can influence mechanics throughout the forearm, wrist, and hand.
For clinicians who rely on sustained precision or pressure with their hands, maintaining mobility along this pathway is essential.
The median nerve originates in the neck, passes beneath the pectoralis minor, and travels down the arm into the carpal tunnel at the wrist.
When the pectoralis minor becomes shortened or compressed, pressure can increase on this nerve as it passes beneath the muscle. As a result, tension may travel down the arm and present as carpal tunnel symptoms at the wrist, even though the contributing restriction may occur higher in the chain.
Keeping this pathway open—from the chest and shoulder through the arm—helps reduce unnecessary compression along the nerve and supports healthier mechanics throughout the upper limb.
Self-Myofascial Release for the Pectoralis Minor

Technique
• Lie on your side with your arm long and straight, positioned under your ear
• Place a small ball in the armpit region — avoid a golf ball or anything very hard, use a pliable rubber or air-filled ball
• Pull the larger pectoralis major tendon out of the way so the ball can contact the tissue beneath it, directly in front of the armpit
• Gently wiggle the ball under the big pectoralis major tendon toward the lateral ribs where the pectoralis minor lies
• Apply light body weight into the ball — you are on your ribs and the pec minor is thin, so keep the pressure gentle
• Breathe slowly and allow the tissue to soften
• Move the ball slightly higher or lower to influence more of the tissue
• Add small arm or rib cage movements to encourage the myofascia to glide, slide, and shear
• Stay below pain — myofascia responds to patience and time, not force
Keeping the Line Open
Releasing the pectoralis minor is only one piece of maintaining this pathway. Clinicians who work with their hands throughout the day must also keep the rest of the line mobile.
Regularly open the chest and shoulder. Stretch the biceps and forearm flexors and gently mobilize your thumb joint.
Together these simple habits help maintain adaptability along the entire Deep Front Arm Line.
When the pathway from chest to thumb remains mobile, load distributes more evenly through the arm. As a result, the wrist does not have to absorb the full burden of repetitive clinical work.
This article focused on the Deep Front Arm Line. For a closer look at how the superficial structures of the chest and arm influence posture and spinal mobility, see the companion article: When Your Work Lives in Front of You — The Superficial Front Arm Line in Clinical Practice.